Facioscapulohumeral Muscular Dystrophy (FSH, FSHD)
Facioscapulohumeral Muscular Dystrophy (FSH, FSHD)
What is facioscapulohumeral muscular dystrophy?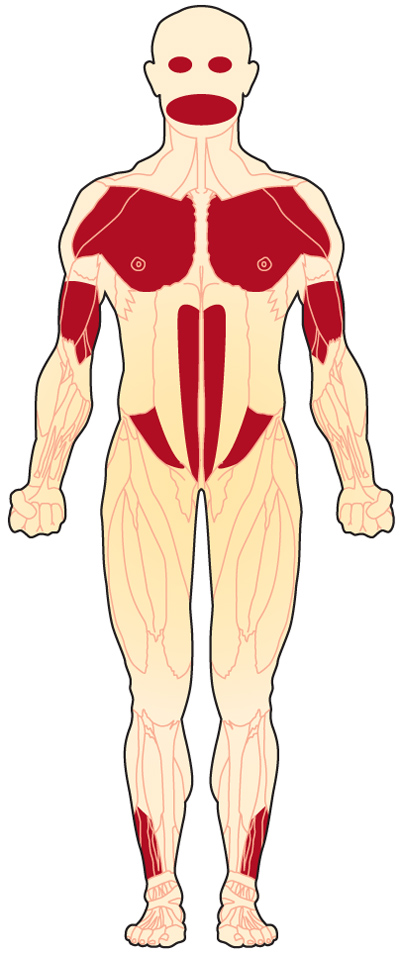
Facioscapulohumeral muscular dystrophy (FSHD) is a genetic muscle disorder in which the muscles of the face, shoulder blades, and upper arms are among the most affected.
The long name comes from facies, the Latin word and medical term for face; scapula, the Latin word and anatomical term for shoulder blade; and humerus, the Latin word for upper arm and the anatomical term for the bone that goes from the shoulder to the elbow.
The term muscular dystrophy means progressive muscle degeneration, with increasing weakness and atrophy (loss of bulk) of muscles. In FSHD, weakness first and most seriously affects the face, shoulders, and upper arms, but the disease usually also causes weakness in other muscles. FSHD is the third most common type of muscular dystrophy, behind Duchenne and Becker muscular dystrophies and myotonic dystrophy. The estimated prevalence of FSHD about 4 cases per 100,000 individuals.1,2,3,4,5
What are the symptoms of FSHD?
In around 90% of FSHD patients, symptoms usually begin before age 20, with weakness and atrophy of the muscles around the eyes and mouth, shoulders, abdominal muscles, upper arms, and lower legs, usually with asymmetric involvement.
Some experts divide FSHD into adult-onset and infantile-onset forms. The adult-onset (which includes FSHD that begins in adolescence) is far more common. In either type of FSHD, facial weakness can start in childhood. Occasionally, other FSHD symptoms appear in early childhood.
Infantile-onset FSHD generally runs a more pronounced course with regard to muscle weakness, and sometimes also affects hearing and vision. Preliminary evidence suggests that the infantile-onset form is associated with a larger piece of missing DNA. For more, see Signs and Symptoms.
What causes FSHD?
FSHD may be inherited through either the father or the mother, or it may occur without a family history. The most probable cause of FSHD is a genetic flaw (mutation) that leads to inappropriate expression of the double homeobox protein 4 gene (DUX4) on chromosome 4, in the 4q35 region.6 The segment is not part of any particular gene, but it nevertheless seems to interfere with the correct processing of genetic material.
For more about the genetic causes of FSHD, see Causes/Inheritance. For more about how the missing chromosome 4 segment may cause FSHD, see Research.
What is the progression of FSHD?
FSHD usually progresses very slowly and rarely affects the heart or respiratory system. Most people with the disease have a normal life span. However, disease severity is highly variable.
What is the status of research in FSHD?
In 2009, MDA-supported researchers found that pieces of a gene called DUX4 are abnormally activated in FSHD-affected cells, leading to production of potentially toxic proteins. Blocking the erroneously activated genes or the proteins made from them seems a likely pathway for the eventual treatment of FSHD. For more, see Research.
Download our Facioscapulohumeral Muscular Dystrophy (FSH, FSHD) Fact Sheet
References
- Understanding Neuromuscular Disease Care. IQVIA Institute. Parsippany, NJ. (2018).
- Mostacciuolo, M. L. et al. Facioscapulohumeral muscular dystrophy: Epidemiological and molecular study in a north-east Italian population sample. Clin. Genet. (2009). doi:10.1111/j.1399-0004.2009.01158.x
- Sposìto, R. et al. Facioscapulohumeral Muscular Dystrophy Type 1A in Northwestern Tuscany: A Molecular Genetics-based Epidemiological and Genotype–Phenotype Study. Genet. Test. (2005). doi:10.1089/gte.2005.9.30
- Flanigan, K. M. et al. Genetic characterization of a large, historically significant Utah kindred with facioscapulohumeral dystrophy. Neuromuscul. Disord. (2001). doi:10.1016/S0960-8966(01)00201-2
- Deenen, J. C. W. et al. EPopulation-based incidence and prevalence of facioscapulohumeral dystrophy. Neurology (2014). doi:10.1212/WNL.0000000000000797
- Gabriëls, J. et al. Nucleotide sequence of the partially deleted D4Z4 locus in a patient with FSHD identifies a putative gene within each 3.3 kb element. Gene (1999). doi:10.1016/S0378-1119(99)00267-X
Looking for more information, support or ways to get involved?
Find MDA
in your Community
-

Grants at a Glance
Read More -

Search for Clinical Trials
Learn More

